
Most of us swallow without thinking—until it starts to feel like food is “sticking,” liquids won’t go down smoothly, or meals become stressful. Achalasia is one of the conditions that can cause this. It’s uncommon, but it can significantly affect nutrition, sleep, and everyday comfort if not recognized early.
If you’re seeking expert evaluation and advanced digestive care, many international patients begin their journey with Liv Hospital, where gastroenterology teams can coordinate precise testing and treatment plans.
What Is Achalasia in Simple Terms?
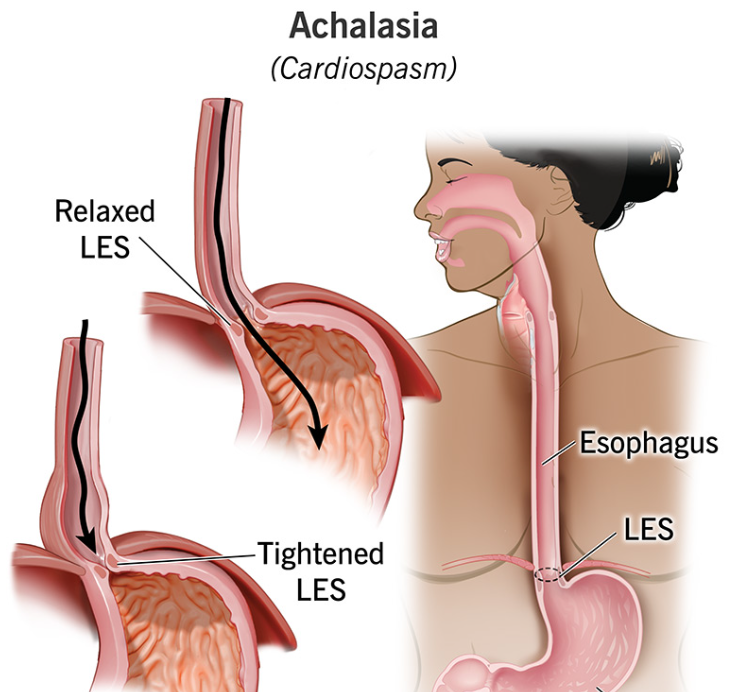
Achalasia is a chronic swallowing disorder where the esophagus (the muscular tube that carries food to the stomach) loses its ability to move food down normally, and the lower esophageal sphincter (LES)—the “valve” at the bottom—doesn’t relax as it should. The result is a functional blockage: food and liquids have trouble passing into the stomach, and the esophagus gradually stretches over time.
It’s not the same as acid reflux. In reflux, the LES is too loose and allows acid upward. In achalasia, the LES is often too tight and prevents contents from moving downward.
Key Signs People Often Ignore (Until They Worsen)
Achalasia typically develops slowly, so it’s easy to dismiss early symptoms as “indigestion” or stress. Common warning signs include:
- Difficulty swallowing solids and liquids (a major clue—many conditions affect solids first, but achalasia often impacts both)
- Regurgitation of undigested food, especially hours after eating
- Chest discomfort or pressure that may mimic heartburn
- Chronic coughing at night or waking up choking (from regurgitation into the airway)
- Unexplained weight loss or avoiding meals because eating feels uncomfortable
- Frequent respiratory infections in some cases, due to aspiration
If symptoms are persistent, the goal isn’t to “wait it out,” but to identify the cause before the esophagus becomes significantly dilated.
Why Achalasia Happens
Achalasia is considered a neuromuscular disorder because the underlying issue is damage to nerves inside the esophageal wall. When these nerves are impaired, the coordinated squeezing motion (peristalsis) becomes ineffective, and the LES fails to open properly during swallowing.
In many patients, a clear single cause isn’t found. What matters clinically is recognizing the pattern early, confirming the diagnosis accurately, and choosing an intervention that reduces the outflow resistance at the LES.
How Doctors Confirm the Diagnosis
Because symptoms can overlap with GERD or strictures, proper testing is essential. A typical evaluation may include:
1) Barium swallow (contrast X-ray)
You drink a contrast liquid, and imaging shows how it moves. Achalasia can show delayed emptying and a tapered narrowing near the LES (often described as a classic “bird-beak” shape).
2) Upper endoscopy (EGD)
This is used to look inside the esophagus and stomach and—very importantly—to rule out “pseudoachalasia,” where another condition (like a narrowing or mass) creates similar symptoms.
3) High-resolution manometry (the most definitive test)
This measures pressure and muscle coordination in the esophagus and is often the test that confirms achalasia and identifies the subtype, which can influence treatment choice.
For a deeper clinical overview and treatment pathways, you can reference GASTROENTEROLOGY Achalasia as a starting point for what patients typically discuss with a specialist.
Achalasia Subtypes: Why the “Type” Matters
Modern manometry helps classify achalasia patterns. In practical terms, subtyping helps predict which treatments may work best.
- Type I (classic): minimal esophageal pressurization—often a more “weak and dilated” esophagus
- Type II: pressurization occurs across the esophagus; this type often responds well to multiple treatment options
- Type III (spastic): abnormal spastic contractions; may need a longer muscle cut during certain procedures
This classification helps specialists match the intervention to the patient’s physiology rather than using a one-size-fits-all approach.
Treatment Options: What Actually Helps
Achalasia can’t be “cured” with a pill because the underlying nerve dysfunction remains. Treatment focuses on reducing the LES barrier, allowing food to pass into the stomach more easily.
Pneumatic dilation
A balloon is inflated at the LES to stretch it open. It can be effective, though some patients need repeat dilations over time.
Surgical myotomy (Heller myotomy)
A surgeon cuts the LES muscle fibers to relieve the functional obstruction. This is often combined with an anti-reflux procedure because lowering LES pressure can increase reflux risk afterward.
POEM (Peroral Endoscopic Myotomy)
A minimally invasive endoscopic technique where the myotomy is performed from inside the esophagus. POEM can be especially useful in spastic patterns and can be tailored in length based on the patient’s motility findings.
The “best” option depends on symptom severity, subtype, anatomy, age, and local expertise—so the decision is usually made after a structured diagnostic workup.
Life After Treatment: What Recovery and Follow-Up Look Like
Most people notice meaningful improvement in swallowing after successful LES-directed therapy. However, follow-up matters because:
- Some patients can develop reflux symptoms after myotomy-based treatments
- Swallowing may improve quickly, but the esophagus may take time to remodel
- Long-standing cases can require ongoing monitoring, particularly if the esophagus became significantly enlarged over many years
Diet adjustments are usually temporary during healing (soft diet progression), and long-term guidance often focuses on eating habits that reduce regurgitation and nighttime symptoms.
Practical Tips That Can Reduce Day-to-Day Discomfort
While you’re awaiting evaluation or recovering, these strategies may help reduce symptoms (they don’t replace treatment, but they can make daily life easier):
- Eat slowly and chew thoroughly
- Avoid late-night meals; stay upright after eating
- Sip warm water with meals (some patients find it helps passage)
- Elevate the head of the bed if nighttime regurgitation occurs
- Track triggers: certain textures (bread, dense meat) may be harder
Supporting Digestive Comfort Beyond Procedures
After achalasia treatment, many people want to rebuild confidence around eating, sleep, and overall wellness. If you’d like supportive lifestyle content for healthy routines and feeling better day-to-day, you can explore practical wellbeing reads on live and feel.