
Barrett Esophagus is not a condition most people feel every day, yet it carries long-term importance because it quietly increases the risk of esophageal cancer. It develops over years of repeated acid exposure, often in people who have lived with chronic heartburn and reflux symptoms and gradually adapted to them. Understanding what Barrett Esophagus means, how it is monitored, and why follow-up matters is essential for protecting future digestive health.
Patients seeking structured reflux evaluation and long-term surveillance often turn to Liv Hospital, where gastroenterology teams focus not only on symptom relief but also on cancer-prevention strategies.
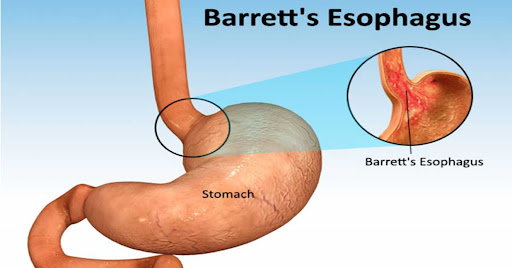
How Barrett Esophagus Develops Over Time
Barrett Esophagus occurs when the normal squamous lining of the lower esophagus is replaced with a different type of tissue that resembles intestinal lining. This transformation is the body’s defensive response to repeated acid injury from chronic gastroesophageal reflux disease (GERD).
Unlike short episodes of heartburn, persistent reflux exposes the esophagus to acid and bile for years. Over time, the tissue adapts to survive this hostile environment. While this adaptation reduces acid damage, it also creates cells that are more vulnerable to abnormal growth.
This is why Barrett Esophagus is described as a pre-cancerous condition—not cancer itself, but a known step along a potential progression pathway.
Why Symptoms Often Don’t Match the Risk
One of the most challenging aspects of Barrett Esophagus is that it usually causes no unique symptoms. Most people feel only typical reflux signs, such as:
- Chronic heartburn
- Regurgitation of acid or food
- Chest discomfort after meals
- Hoarseness or chronic cough
Some patients experience fewer symptoms over time because the altered tissue becomes less sensitive to acid. Unfortunately, symptom improvement does not mean the condition has resolved. This is why Barrett Esophagus is often discovered incidentally during an endoscopy performed for long-standing reflux.
Barrett Esophagus Is Not the Same as GERD
It is important to separate cause from consequence. GERD is the ongoing reflux of stomach acid into the esophagus, while Barrett Esophagus is a structural change that can result from years of untreated or poorly controlled reflux.
Once Barrett Esophagus develops, controlling reflux remains essential, but medication alone does not reverse the cellular change. Instead, management focuses on risk reduction and early detection of dangerous progression.
Understanding Dysplasia and Cancer Risk
Doctors classify Barrett Esophagus based on whether abnormal cells show signs of instability, a process called dysplasia.
- Non-dysplastic Barrett Esophagus: Cell changes are present but stable, with low short-term cancer risk.
- Low-grade dysplasia: Early cellular abnormalities suggest increased cancer potential.
- High-grade dysplasia: Cells are severely abnormal and close to becoming cancerous.
This classification determines how often surveillance is required and whether active treatment is needed. More detailed information on diagnostic classification and treatment pathways is available through GASTROENTEROLOGY Barrett Esophagus, which outlines how risk is stratified and managed.
How Barrett Esophagus Is Diagnosed and Monitored
The diagnosis of Barrett Esophagus is made during an upper endoscopy, where a gastroenterologist visually inspects the esophagus and takes tissue samples (biopsies). These samples are examined under a microscope to confirm the diagnosis and determine whether dysplasia is present.
Monitoring does not stop after diagnosis. Patients typically enter a structured surveillance program involving periodic endoscopies, allowing doctors to detect progression at its earliest, most treatable stage.
Treatment Goals Beyond Medication
Treatment does not aim to “cure” Barrett Esophagus in the traditional sense, but rather to:
- Control acid reflux
- Prevent progression to cancer
- Remove or destroy high-risk tissue when necessary
For patients with dysplasia, advanced endoscopic therapies such as radiofrequency ablation or endoscopic mucosal resection may be recommended. These minimally invasive techniques remove abnormal cells while preserving the rest of the esophagus.
Why Long-Term Follow-Up Matters
Esophageal adenocarcinoma is an aggressive cancer with poor outcomes when detected late. Barrett Esophagus offers a rare opportunity in medicine: a known warning stage that allows doctors to intervene before cancer develops.
Consistent follow-up, medication adherence, and lifestyle adjustments together form the foundation of effective long-term management.
Supporting Digestive Health After Diagnosis
Living with Barrett Esophagus often encourages people to rethink daily habits that influence reflux, such as meal timing, posture after eating, sleep position, and stress management. Small, consistent changes can significantly support medical treatment and improve overall comfort. For broader wellness guidance that complements digestive care, many patients explore lifestyle-focused resources like live and feel as part of a balanced, long-term health approach.